This project was led by Jesse Knight, and published in Epidemics.
Why did we conduct this study?
Access to treatment among people living with HIV in Sub-Saharan Africa has increased substantially since the early 2000s, especially after research showed that being on effective treatment can prevent onward transmission (“undetectable = untransmittable”). At the same time, mathematical models of HIV transmission have been used to predict how many new infections could be averted by scaling-up treatment. However, many models overlook important details about differences in HIV risk within a population, such as differences in sexual activity and changes in sexual activity over time; these details likely influence the predicted number of HIV infections averted by treatment scale-up.
What did we do?
We systematically reviewed all existing studies where mathematical models of HIV transmission were used to simulate scale-up of HIV treatment. For each study, we recorded if and how different details were included in the model. We recorded details related to:
- HIV biology, including acute infection, late-stage infection, drug resistance’
- Changes to behaviour among people living with HIV, due to HIV symptoms or diagnosis
- Sexual activity, including different “activity groups”, specific “key populations” like men who have sex with men and female sex workers, changes in sexual activity over time, different types of sexual partnerships, who has sex with whom, and
- Differences in treatment coverage across any sub-groups of people living with HIV
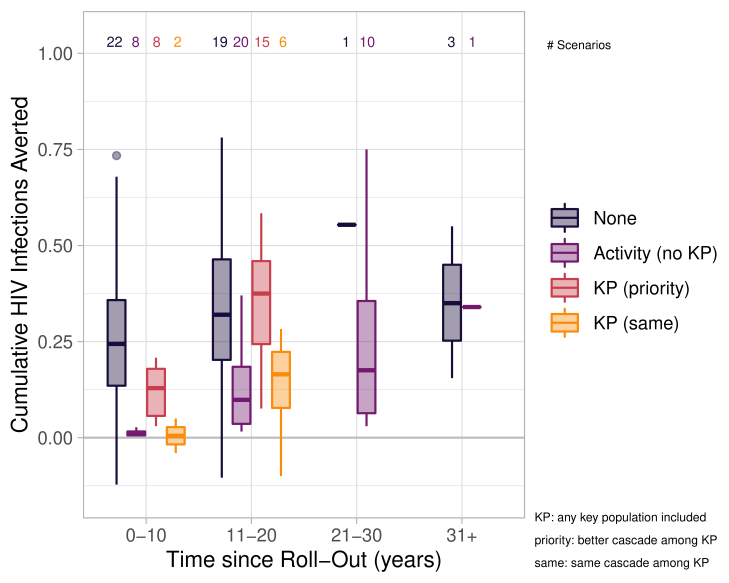
For each study, we also recorded the percentage of future infections predicted to be averted through treatment scale-up; studies often included multiple scenarios, so we recorded results from each scenario separately. Finally, we statistically tested whether the predicted infections averted by treatment were different (on average) depending on if/how each detail was included in a given model.
What did we find?
Of 94 studies we reviewed, we found that only:
- 64 included any differences in sexual activity
- 39 included any key populations
- 28 included any change in sexual activity over time, and
- 21 included any differences in treatment coverage across sub-groups
Moreover, our statistical test suggested that models could predict significantly different numbers of infections averted through treatment depending on whether or not the model included changes in sexual activity over time, and any differences in treatment coverage across sub-groups.
We also found that no studies explored scenarios where treatment coverage was lower among key populations, although this may be true in many places.
What do these findings mean for public health?
Models of HIV transmission are widely used for predicting the impact of HIV treatment scale-up. To avoid biased predictions, modellers should try to include the key details we identified, namely: changes in sexual activity over time, and differences in treatment coverage across sub-groups, especially key populations.
This research was supported by the Natural Sciences and Engineering Research Council of Canada (NSERC CGS-D), an Ontario Early Researcher Award (ER17-13-043), and the Canadian Institutes of Health Research Foundation (FN-13455).
